What Is Acute Metabolic Encephalopathy?
Acute metabolic encephalopathy is a reversible, diffuse brain dysfunction caused by systemic metabolic disturbances rather than structural brain disease. It presents clinically with altered mental status, confusion, reduced consciousness, or cognitive impairment.
In the ICD-10-CM classification system, metabolic encephalopathy is categorized under neurological disorders and is coded based on physician documentation and underlying etiology.
From a medical coding perspective, acute metabolic encephalopathy is not a symptom—it is a distinct clinical diagnosis that often qualifies as a Major Complication or Comorbidity (MCC) when documented and coded correctly.
Symptoms and Clinical Presentation of Metabolic Encephalopathy
Acute metabolic encephalopathy presents with a wide range of neurological symptoms depending on the severity and underlying cause.
Common Symptoms
– Confusion or disorientation
– Altered level of consciousness
– Agitation or lethargy
– Memory impairment
– Difficulty concentrating
Why Symptoms Matter for Coders
While symptoms alone are not sufficient for ICD-10 coding, they support the medical necessity and clinical validity of the documented diagnosis.
Coders should ensure that the documented diagnosis of metabolic encephalopathy aligns with the patient’s clinical presentation and treatment course.
How Clinical Diagnosis Translates Into ICD-10 Coding
In clinical practice, physicians diagnose metabolic encephalopathy based on patient symptoms, laboratory findings, and underlying conditions.
However, in medical coding, the diagnosis must be explicitly documented and clearly linked to its cause.
This distinction is important because:
– Clinical suspicion alone does not support code assignment
– Coders cannot infer diagnoses without provider documentation
– Accurate coding depends on clear cause-and-effect relationships
Bridging the gap between clinical diagnosis and coding ensures both compliance and accurate reimbursement.
Key Clinical and Coding Characteristics
Type of condition: Neurological dysfunction
Cause: Metabolic imbalance (e.g., hyponatremia, uremia, hypoglycemia)
Reversibility: Often reversible with treatment of the underlying cause
Coding requirement: Must be explicitly documented by the physician
Reimbursement impact: Frequently classified as an MCC in inpatient coding
Understanding these attributes is essential because ICD-10 coding depends not just on clinical findings but on how the condition is documented and linked to its underlying cause.
A hospitalist sees a patient who was admitted overnight with an altered mental status. Lab work showed severe electrolyte imbalances. A consult note from neurology describes acute metabolic encephalopathy secondary to hyponatremia. The hospitalist documents the same in their daily progress note. Now the coder has to assign an ICD-10 code.
The coder types encephalopathy into the search field. Several options appear. G93.41 shows up. So does G92.9. And there is a reference pointing toward a combination approach where the underlying metabolic cause gets coded separately. The coder picks G93.41 and moves on.
G93.41 is correct only when metabolic encephalopathy is clearly documented and supported by clinical findings. Or it might not be, depending on whether the encephalopathy was toxic-metabolic, whether the hyponatremia should also be coded, and whether the physician’s exact language in the note matches the code descriptor. Encephalopathy coding in ICD-10 is one of those areas where the right answer depends heavily on what the physician wrote and how the code set is structured.
This guide covers the ICD-10 codes used for acute metabolic encephalopathy, when each applies, what the documentation needs to say, how the condition is coded alongside its underlying causes, and where coding errors tend to occur in inpatient and outpatient settings.
How Acute Metabolic Encephalopathy Is Classified in ICD-10
ICD-10 does not assign a single universal code for all types of encephalopathy. Instead, encephalopathy is classified based on its underlying mechanism, such as metabolic, toxic, or structural causes.
For accurate coding, it is essential to distinguish between these types because each category maps to a different code range and has different sequencing and reimbursement implications.
The following sections break down the most relevant ICD-10 codes used in clinical practice and explain when each should be applied.

Encephalopathy does not have a single ICD-10 code. It has a family of codes spread across different chapters depending on the type and cause. Understanding where each code lives and what distinguishes it from the others is the foundation of accurate encephalopathy coding.

G93.41: Metabolic Encephalopathy
G93.41 is the code for metabolic encephalopathy. This was added to ICD-10-CM in 2017 after the previous coding approach used a general unspecified encephalopathy code that did not capture metabolic presentations specifically. G93.41 applies when the physician has documented metabolic encephalopathy as the diagnosis, whether described as acute metabolic encephalopathy, toxic-metabolic encephalopathy, or simply metabolic encephalopathy.
The code sits in Chapter 6, Diseases of the Nervous System, under the other disorders of the brain category G93. It is not a residual or unspecified code. It describes a specific type of encephalopathy tied to metabolic dysfunction rather than structural brain disease, infection, or toxic agent.
When a physician documents acute metabolic encephalopathy, G93.41 is the primary encephalopathy code. The metabolic cause, whether it is hyponatremia, hyperammonemia, uremia, hepatic failure, hypoglycemia, or another metabolic disturbance, gets coded separately as an additional diagnosis. ICD-10 does not combine the encephalopathy and its cause into a single code for most metabolic presentations. Both need to appear on the claim.
G92.9: Unspecified Toxic Encephalopathy
G92.9 covers toxic encephalopathy, unspecified. This code applies when the encephalopathy was caused by a toxic agent rather than a purely metabolic disturbance. Drug-induced encephalopathy, encephalopathy from heavy metal toxicity, and encephalopathy secondary to exposure to industrial chemicals would use codes in the G92 range rather than G93.41.
G92.9 is the unspecified version. G92.8 covers other toxic encephalopathies. When a physician documents toxic-metabolic encephalopathy without clearly distinguishing the toxic component from the metabolic component, the coder is in a gray area where a physician query may be appropriate. Toxic-metabolic is a clinical term that blends two mechanisms. Whether it codes to G92 or G93.41 depends on which component is primary in the physician’s documentation.
G92.0: Immune Effector Cell-Associated Neurotoxicity Syndrome
G92.0 was added in 2023 to capture ICANS, the neurological complication of CAR-T cell therapy. This is a specific code for a specific clinical scenario and should not be confused with general toxic or metabolic encephalopathy. It is mentioned here only because it added a new code to the G92 range that coders should be aware of when working in oncology settings where CAR-T therapy is administered.
G93.49: Other Encephalopathy
G93.49 covers other encephalopathies that do not fall into the metabolic category and do not fit a more specific code. Hypertensive encephalopathy, for example, used to be coded here before it received its own code. This is a residual category and should not be the default choice when a more specific code exists.
F05: Delirium Due to Known Physiological Condition
This code comes up frequently in the encephalopathy discussion because clinically, acute metabolic encephalopathy and delirium are often intertwined. When a physician documents delirium as the clinical presentation and identifies the metabolic cause as the physiological basis, F05 is the code for the delirium component. F05 and G93.41 can both appear on the same claim when both are documented, but their relationship needs to be clear in the documentation.
Difference Between Metabolic, Toxic, and Delirium-Related Encephalopathy
Accurate ICD-10 coding depends on distinguishing between different types of encephalopathy, as each has separate classification rules.
Metabolic Encephalopathy (G93.41)
– Caused by internal metabolic imbalances
– Examples: hyponatremia, uremia, hypoglycemia
– Requires separate coding of the underlying cause
Toxic Encephalopathy (G92.9, G92.8)
– Caused by external toxins or substances
– Examples: drug toxicity, heavy metals, chemicals
– May require additional poisoning or adverse effect codes
Delirium (F05)
– Represents a clinical syndrome rather than a specific neurological pathology
– Often overlaps with metabolic encephalopathy
– Can be coded alongside G93.41 when both are documented
Why This Distinction Matters
Misclassifying encephalopathy can lead to:
– Incorrect code assignment
– Lost MCC opportunities
– Compliance risks in audits
Coders should rely on physician documentation and query when terminology such as “toxic-metabolic encephalopathy” creates ambiguity.
When Acute Metabolic Encephalopathy Gets Coded as a Principal Diagnosis
In the inpatient setting, the principal diagnosis is the condition established after study to be chiefly responsible for the admission. Whether acute metabolic encephalopathy can serve as the principal diagnosis depends on what brought the patient to the hospital.
When a patient presents primarily with altered mental status, confusion, or decreased level of consciousness and the workup identifies metabolic encephalopathy as the explanation, G93.41 may appropriately be the principal diagnosis. The metabolic cause codes alongside it as an additional diagnosis.
When the patient was admitted for a primary condition such as sepsis, liver failure, or severe hyponatremia, and the encephalopathy developed as a consequence of that primary condition, the primary condition sequences first. G93.41 becomes a secondary diagnosis coded as a complication or comorbidity that affected the hospital course.
This sequencing distinction matters significantly for DRG assignment. Acute metabolic encephalopathy coded as a secondary diagnosis alongside sepsis, for example, qualifies as a Major Complication or Comorbidity under the MS-DRG system. That MCC designation moves the case to a higher-weight DRG tier and increases reimbursement. Skipping G93.41 as a secondary diagnosis because the encephalopathy resolved or because it seemed like a symptom of the primary condition means losing that MCC impact.
Since ICD-10 requires separate reporting of the underlying metabolic disturbance, understanding these causes is essential for accurate code assignment and sequencing.
Coding the Underlying Metabolic Cause Alongside G93.41
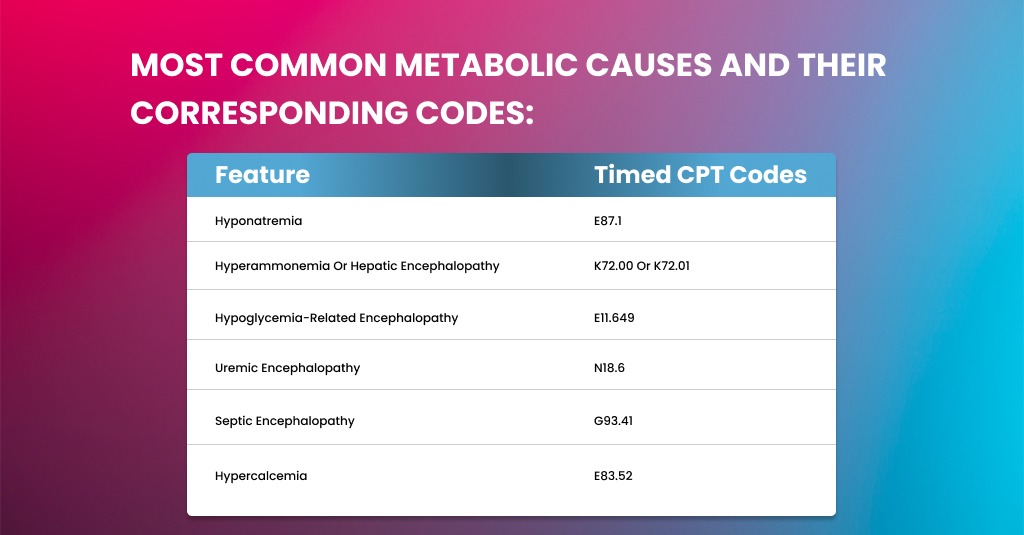
G93.41 describes the neurological consequence. The underlying metabolic disturbance is coded separately. These are the most common metabolic causes and their corresponding codes:
- Hyponatremia: E87.1. When acute hyponatremia causes encephalopathy, both G93.41 and E87.1 are coded. Sequence based on what was the principal reason for the admission.
- Hyperammonemia or hepatic encephalopathy: K72.00 or K72.01 for acute hepatic failure, or K72.10 for chronic hepatic failure. For hepatic encephalopathy specifically, some coders and clinicians use G93.41 alongside the hepatic failure code. Others argue that hepatic encephalopathy is better captured by the K72 codes with an instructional note. Physician documentation determines the approach.
- Hypoglycemia-related encephalopathy: E11.649 for diabetic hypoglycemia without coma, or the appropriate E-code depending on the type of diabetes and severity. The encephalopathy from hypoglycemia is a severe presentation that warrants specific coding of both the glucose disturbance and the neurological consequence.
- Uremic encephalopathy: N18.6 for end-stage renal disease or the applicable N18 CKD stage code, alongside G93.41 for the encephalopathy. Uremic encephalopathy is a serious complication of renal failure and should be coded as such.
- Septic encephalopathy: When sepsis causes metabolic encephalopathy, the sepsis code sequences first. G93.41 follows as a complication of the sepsis. Septic encephalopathy is a recognized complication that carries MCC status in DRG assignment.
- Hypercalcemia: E83.52, coded alongside G93.41 when hypercalcemia is the documented metabolic cause.
Documentation Requirements That Support G93.41
The code is valid only when the physician has explicitly documented the diagnosis. This is worth stating clearly because encephalopathy is sometimes implied by clinical findings in the chart without being named as a diagnosis by the treating physician.
A chart that shows altered mental status, abnormal EEG findings, and lab values consistent with metabolic disturbance does not automatically support G93.41 if the physician never documented the diagnosis. The treating physician, consulting physician, or attending must have written acute metabolic encephalopathy, toxic-metabolic encephalopathy, or metabolic encephalopathy in the note. A coder who assigns G93.41 based on clinical inference without physician documentation is coding a condition the physician did not diagnose.
- A named diagnosis of metabolic encephalopathy or acute metabolic encephalopathy in the assessment or discharge summary.
- The identified metabolic cause is documented as the etiology of the encephalopathy.
- Clinical presentation: altered mental status, confusion, decreased responsiveness, or other neurological changes that reflect the encephalopathy.
- Any workup performed to evaluate or rule out other causes of altered mental status: imaging, EEG, CSF analysis, or metabolic panel results.
- Treatment directed at the encephalopathy or its metabolic cause, which demonstrates that the condition affected the management of the patient.
- Outcome: whether the encephalopathy resolved, improved, or persisted at the time of discharge.
Step-by-Step Coding Workflow for Acute Metabolic Encephalopathy
Accurate coding of acute metabolic encephalopathy requires a structured approach.
Step 1: Confirm Physician Documentation
Verify that the provider explicitly documented “metabolic encephalopathy.”
Step 2: Identify the Underlying Cause
Determine the metabolic condition responsible (e.g., hyponatremia, sepsis, renal failure).
Step 3: Assign the Correct Encephalopathy Code
Use G93.41 when metabolic encephalopathy is documented.
Step 4: Code the Underlying Condition
Assign additional codes for the metabolic cause.
Step 5: Determine Sequencing
– Principal diagnosis: based on reason for admission
– Secondary diagnosis: if encephalopathy is a complication
Step 6: Validate MCC Impact
Check whether G93.41 qualifies as MCC for DRG optimization.
Following this structured workflow reduces coding errors and ensures accurate reimbursement.
How G93.41 Affects DRG Assignment and Reimbursement
Acute metabolic encephalopathy qualifies as a Major Complication or Comorbidity under the CMS MS-DRG system in most clinical contexts. When it is coded as a secondary diagnosis on a hospital claim, it moves the case from the base DRG tier to the MCC tier, which typically increases reimbursement by several thousand dollars per admission, depending on the DRG family.
For example, an admission for severe sepsis without any MCC diagnosis codes to a base DRG. Add G93.41 as a secondary diagnosis for a documented complication of septic encephalopathy, and the case moves to the MCC tier. The reimbursement difference can be $3,000 to $7,000, depending on the specific DRG and the hospital’s base payment rate.
This is why secondary diagnosis capture matters so much in hospital medicine coding. The physicians treating these patients are managing real clinical complexity. The documentation often reflects that complexity. The coding has to capture it, or the reimbursement does not reflect what the clinical situation actually was.
Is G93.41 Considered an MCC?
Yes, G93.41 (metabolic encephalopathy) is classified as a Major Complication or Comorbidity (MCC) under the MS-DRG system in most inpatient scenarios.
When documented and coded as a secondary diagnosis, it can significantly increase reimbursement by shifting the case into a higher-weight DRG.
Can Acute Metabolic Encephalopathy Be the Principal Diagnosis?
Acute metabolic encephalopathy can be the principal diagnosis when it is the primary reason for admission, such as in patients presenting with altered mental status due to metabolic imbalance.
However, if the encephalopathy is caused by another primary condition (e.g., sepsis, liver failure), the underlying condition is sequenced first.
What Is the Difference Between G93.41 and G92.9?
– G93.41 is used for metabolic encephalopathy caused by internal physiological disturbances.
– G92.9 is used for toxic encephalopathy caused by external substances.
Choosing the correct code depends entirely on the physician’s documentation of the underlying cause.
Common Coding Errors with Acute Metabolic Encephalopathy
- Using G93.49 instead of G93.41. G93.49 is the other encephalopathy code and should not be used when metabolic encephalopathy is specifically documented. G93.41 is the right code for any metabolic presentation. If the system’s search results return G93.49 as the first result, update the search or lookup.
- Coding only the metabolic cause without G93.41. A claim that includes severe hyponatremia but not the resulting encephalopathy is understating the clinical picture. Both conditions should be coded when both are documented.
- Not coding G93.41 as a secondary diagnosis because it resolved. A condition that resolved during the hospital stay is still coded as a secondary diagnosis if it affected management. Resolved metabolic encephalopathy that prompted a neurology consult, monitoring in the ICU, or medication adjustments was actively managed and belongs on the claim.
- Confusing G93.41 with hepatic encephalopathy. When the physician specifically documents hepatic encephalopathy, the coding approach may differ because hepatic failure codes in the K72 range have their own guidance about when encephalopathy is implied in the code versus when it should be additionally coded. Review the instructional notes in the Tabular for K72 before defaulting to G93.41 for all liver-related encephalopathy.
- Missing the physician documentation requirement. G93.41 cannot be assigned from clinical data alone. The physician must have documented the diagnosis. When the diagnosis is implied but not stated, a physician query is the correct next step, not assigning the code based on clinical judgment.
Why Accurate Encephalopathy Coding Matters for Medical Billing Teams
For hospital coding professionals, CDI specialists, and revenue cycle teams, acute metabolic encephalopathy represents a high-impact diagnosis.
When properly documented and coded:
- It reflects the true severity of illness (SOI)
- It improves risk adjustment and quality reporting
- It increases reimbursement through MCC classification
- It supports audit defensibility and compliance
Failure to capture encephalopathy accurately can result in undercoding, lost revenue, and inaccurate representation of patient complexity.
From a revenue cycle perspective, this makes encephalopathy one of the most important secondary diagnoses to monitor in inpatient coding workflows.
Related Conditions That May Affect Encephalopathy Coding
Metabolic encephalopathy often overlaps with other clinical conditions that can influence coding decisions, including:
– Sepsis-associated encephalopathy
– Hepatic encephalopathy
– Drug-induced neurotoxicity
– Electrolyte imbalances
Understanding these related conditions helps coders make accurate distinctions and avoid misclassification.
Final Thoughts
Acute metabolic encephalopathy coding looks straightforward until you are in the middle of a complex inpatient case with multiple contributing factors, two consulting physicians using different terminology, and a discharge summary that does not connect the clinical dots as clearly as a coder would hope. Getting the code right means knowing the code family, understanding when physician documentation is sufficient versus when a query is needed, and capturing both the encephalopathy and its metabolic cause on the claim. When all of that comes together, the coding accurately reflects what the patient experienced, and the claim correctly represents the clinical complexity that was managed.
Optimize Your Medical Coding Accuracy with A2Z Medical Billing Services
Accurate coding of complex conditions like acute metabolic encephalopathy requires more than just knowledge of ICD-10—it requires clinical insight, documentation expertise, and a deep understanding of reimbursement systems.
At A2Z Medical Billing Services, we support healthcare providers across high-impact specialties such as hospital medicine, critical care, nephrology, and internal medicine—where conditions like metabolic encephalopathy are frequently encountered and often affect reimbursement.
Our certified coding specialists help you:
- Capture high-value diagnoses such as MCC conditions (e.g., G93.41)
- Improve clinical documentation accuracy across inpatient and specialty care settings
- Ensure proper sequencing of complex diagnoses
- Reduce claim denials and audit risks
- Maximize reimbursement through accurate DRG optimization
Whether you manage inpatient services, specialty practices, or multi-provider groups, our team ensures your coding reflects the true clinical complexity of your cases.
Contact A2Z Medical Billing Services today to improve coding accuracy, compliance, and revenue performance.
FAQ
Can Metabolic Encephalopathy Be Coded Without an Underlying Cause?
No, ICD-10 requires that the underlying metabolic cause be identified and coded alongside G93.41 whenever documented.
When Should a Physician Query Be Raised for Encephalopathy?
A physician query should be raised when documentation is unclear, conflicting, or does not specify whether encephalopathy is metabolic, toxic, or another type.
Does Metabolic Encephalopathy Always Qualify as MCC?
In most inpatient cases, metabolic encephalopathy qualifies as an MCC, but this depends on payer guidelines and case context.