Urinary tract infections (UTIs) might sound routine, but when it comes to billing and coding, they’re anything but. From distinguishing between a lower UTI and pyelonephritis to documenting symptoms correctly for payers, getting the ICD-10 right can make or break your reimbursement.
This guide will walk you through everything you need to know — from the correct ICD-10-CM codes to documentation tips, CPT pairings, and best billing practices to keep your claims clean and compliant.
Understanding Urinary Tract Infections UTI
Before we jump into coding, let’s revisit what a UTI really is.
A urinary tract infection is an infection that affects any part of the urinary system — kidneys, bladder, ureters, or urethra. Most infections involve the lower urinary tract (the bladder and urethra).
UTIs are extremely common — particularly among women. According to CDC data, about 50–60% of women will experience at least one UTI in their lifetime, and nearly 10 million clinical visits per year in the U.S. are related to UTIs.
From a coding standpoint, specificity is everything. Coding just “UTI” is vague. You need to identify:
- The site of infection (e.g., bladder, urethra, kidney)
- Whether it’s acute or chronic
- If it’s recurrent
- If it’s associated with another condition (like pregnancy, catheter use, or obstruction)
That’s how you go from a deniable claim to a fully reimbursable one.
ICD-10-CM Codes for UTIs (Main Categories)
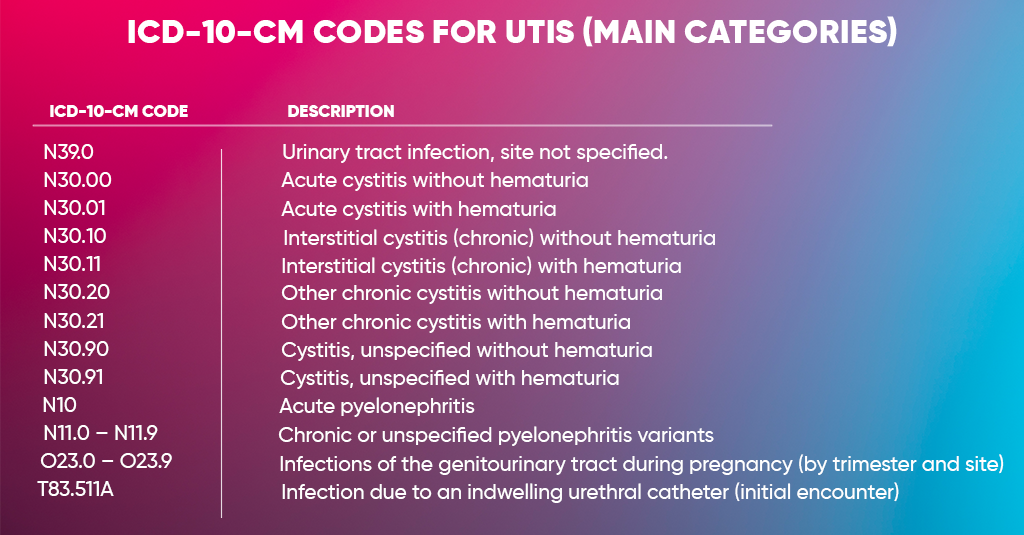
UTIs fall under Chapter 14 of ICD-10-CM:
Diseases of the Genitourinary System (N00–N99)
Here are the key codes you’ll use most often:
| ICD-10-CM Code | Description |
| N39.0 | Urinary tract infection, site not specified. |
| N30.00 | Acute cystitis without hematuria |
| N30.01 | Acute cystitis with hematuria |
| N30.10 | Interstitial cystitis (chronic) without hematuria |
| N30.11 | Interstitial cystitis (chronic) with hematuria |
| N30.20 | Other chronic cystitis without hematuria |
| N30.21 | Other chronic cystitis with hematuria |
| N30.90 | Cystitis, unspecified without hematuria |
| N30.91 | Cystitis, unspecified with hematuria |
| N10 | Acute pyelonephritis |
| N11.0 – N11.9 | Chronic or unspecified pyelonephritis variants |
| O23.0 – O23.9 | Infections of the genitourinary tract during pregnancy (by trimester and site) |
| T83.511A | Infection due to an indwelling urethral catheter (initial encounter) |
Documentation Essentials for UTI Coding
Here’s what your documentation should always include for clean, compliant billing:
A. Site of Infection
- Bladder, kidney, urethra, or unspecified.
B. Type of Infection
- Acute, chronic, recurrent, or secondary (e.g., catheter-associated).
C. Causative Organism (if known)
- Use additional B95–B97 codes for organism identification.
Examples:
- B96.20 – E. coli as cause of disease classified elsewhere
- B96.4 – Proteus (mirabilis) as cause of disease classified elsewhere
D. Associated Conditions
- Pregnancy (O23.x)
- Catheter presence (T83.5x)
- Obstruction or stones (N20.x)
- Diabetes (E11.9)
E. Complications or Severity
- Hematuria
- Sepsis
- Pyelonephritis
Common CPT Codes Used with UTI Diagnoses
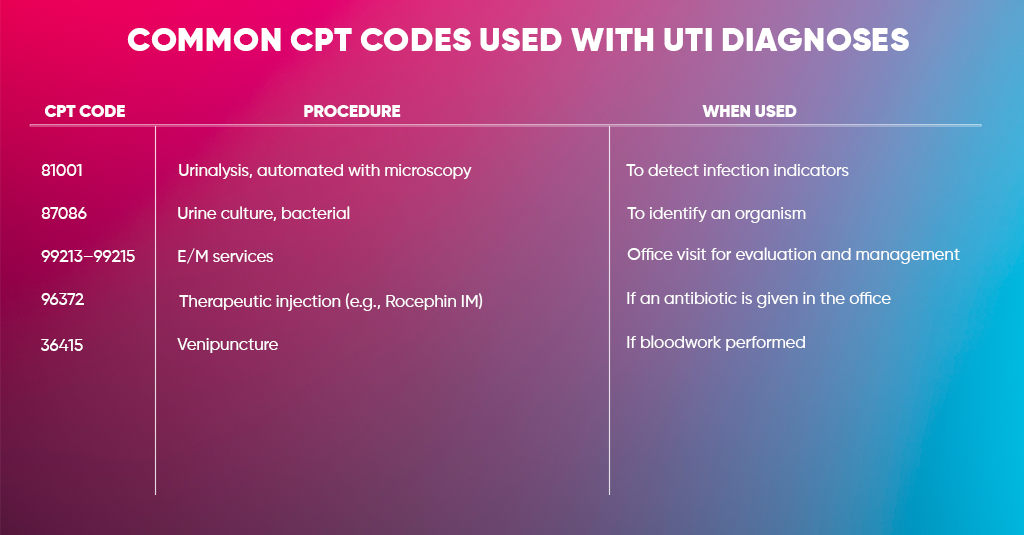
| CPT Code | Procedure | When Used |
| 81001 | Urinalysis, automated with microscopy | To detect infection indicators |
| 87086 | Urine culture, bacterial | To identify an organism |
| 99213–99215 | E/M services | Office visit for evaluation and management |
| 96372 | Therapeutic injection (e.g., Rocephin IM) | If an antibiotic is given in the office |
| 36415 | Venipuncture | If bloodwork performed |
Billing and Reimbursement Guidelines
Billing for UTIs may seem simple at first glance, but minor coding errors or missing documentation can easily delay or reduce reimbursement. Since UTI claims often depend on factors like infection type, location, and patient condition (acute vs. chronic), accuracy is everything. Properly pairing diagnosis codes with the right CPT and modifiers not only prevents denials but also ensures full compliance with payer rules.
Here’s what every provider and biller should focus on:
Code to the Highest Specificity
UTI coding isn’t a “one-size-fits-all” situation. Always identify where the infection is located. For instance:
- N30.0–N30.9 covers bladder infections (cystitis).
- N10–N12 relates to kidney infections (pyelonephritis).
- N39.0 is for UTIs where the site isn’t specified.
Payers don’t like vague or general codes. If your documentation doesn’t state the exact infection site, the claim may be questioned or reimbursed at a lower rate. So, always code based on the most specific and confirmed diagnosis documented by the provider.
Link Diagnosis with Correct CPT Codes
Each ICD-10 diagnosis must logically support the service or test billed. For example, if you’re billing for a urinalysis (CPT 81003) or urine culture (CPT 87086), your diagnosis code should indicate a UTI or urinary symptoms that justify why that test was done.
If you use a UTI code but bill unrelated procedures — say, an EKG — without a clinical reason, payers might flag it. Think of CPT codes as “what you did” and ICD-10 codes as “why you did it.” Both need to match for successful reimbursement.
Avoid Unspecified Codes When Possible
Using N39.0 (UTI, site not specified) is acceptable only when documentation truly lacks detail or the infection site hasn’t been identified yet. However, overusing unspecified codes signals weak documentation to payers and may lead to payment reductions or denials.
Encourage providers to document symptoms and findings precisely. For example, instead of “UTI,” note “acute cystitis” or “acute pyelonephritis.” This small step can significantly improve claim accuracy and reimbursement rates.
Verify Medical Necessity
Insurance payers won’t reimburse a claim unless the documentation proves the test or treatment was medically necessary. Always include supporting evidence like:
- Urinalysis and culture reports
- Symptoms (pain, burning, frequency, fever)
- Physician notes describing diagnosis and plan of care
The more complete your chart, the stronger your justification for reimbursement. Medicare and commercial payers both audit this closely.
Check Payer-Specific Policies
Each payer has its quirks. Medicare, Medicaid, and commercial insurers often differ in how they cover UTI testing, antibiotic use, or repeat cultures. For example, some payers may limit urine cultures to once every few days unless documentation explains the reason for repeat testing.
Before submitting, confirm your payer’s Local Coverage Determination (LCD) or policy guidelines to ensure your claim meets all conditions for payment.
Use Modifiers Correctly
When billing multiple services on the same date — like an office visit plus a urinalysis — you may need to add modifiers. For instance:
- Modifier 25: Use when an E/M service is performed on the same day as a procedure, and both are separately identifiable.
- Modifier 59: Use to show distinct, non-overlapping services that shouldn’t be bundled.
Incorrect or missing modifiers can cause “duplicate” or “bundled” claim denials.
Keep Documentation Consistent
Your clinical documentation should always mirror your billing claim. If your note says “bladder infection,” but your claim lists N39.0 (site unspecified), that mismatch can raise red flags for an audit.
Everything — symptoms, test results, prescriptions — should tell one clear story that supports the diagnosis and billed services. Consistency is your best defense against recoupments or compliance issues.
Review Claim Frequency and Recurrence
Frequent UTI claims for the same patient within a short period can trigger payer scrutiny. They might question whether each episode is truly new or part of a chronic condition.
If the infection returns, document clearly whether it’s a recurrent UTI or follow-up care for a previous infection. Use terms like “new episode” or “persistent symptoms” to support medical necessity and avoid duplicate billing denials.
Track Denial Patterns
If you’re seeing repeated denials for UTI claims — for reasons like “diagnosis missing,” “not medically necessary,” or “invalid code combination” — don’t just resubmit mindlessly. Investigate the root cause.
Run a monthly or quarterly denial report, identify patterns, and retrain staff if needed. Often, a minor fix in documentation or coding workflow (like adding infection site details) can drastically cut down rejections and speed up payments.
Final Thoughts
Urinary Tract Infections may be one of the most common diagnoses in clinical practice, but billing for them is anything but routine. One missing detail — whether it’s the site of infection, the presence of symptoms, or the right CPT pairing — can easily turn a simple claim into a frustrating denial. The secret to smooth reimbursement lies in getting the documentation, coding, and medical necessity right the first time.
Always remember: accuracy and specificity protect your revenue. Make sure your notes clearly describe the infection site (bladder, kidney, or urinary tract), justify each lab or test, and use the ICD-10 code that fits the exact scenario. Keep your billing staff updated on payer rules, and review any recurring denial trends before they start affecting cash flow.
Let Our Certified Medical Billing Team Streamline Your UTI Claims
If UTI billing keeps draining your revenue instead of boosting it, it’s time to call in the experts. At A2Z Medical Billing Experts, we handle everything from A to Z — eligibility checks, coding precision, denial prevention, and compliance audits. We know every nuance of ICD-10 codes like N39.0, N30.01, and N10, and how to make them pay faster.