Graves’ disease looks simple on paper: an overactive thyroid. But in medical billing, it behaves like a small, stubborn labyrinth. A single wrong code, a missing lab result, or an ignored payer rule can turn a routine office visit into a denied claim and a slow-paying headache.
If you’re a physician, coder, or billing manager, mastering the correct ICD-10 codes for graves, documentation points, and claim workflow isn’t optional. It’s how you protect revenue and patient care. Read on:
Let’s go through the practical steps that turn messy claims into clean, paid ones.
What Is Graves’ Disease?
Graves’ disease is an autoimmune disorder where the immune system attacks the thyroid, leading to hyperthyroidism (an overactive thyroid).
Common symptoms include anxiety, weight loss, tremors, and bulging eyes (Graves’ ophthalmopathy).
From a clinical standpoint, this condition can affect multiple systems, so coding requires specificity — not just “hyperthyroidism,” but the type, manifestations, and complications.
ICD-10 Codes for Graves’ Disease
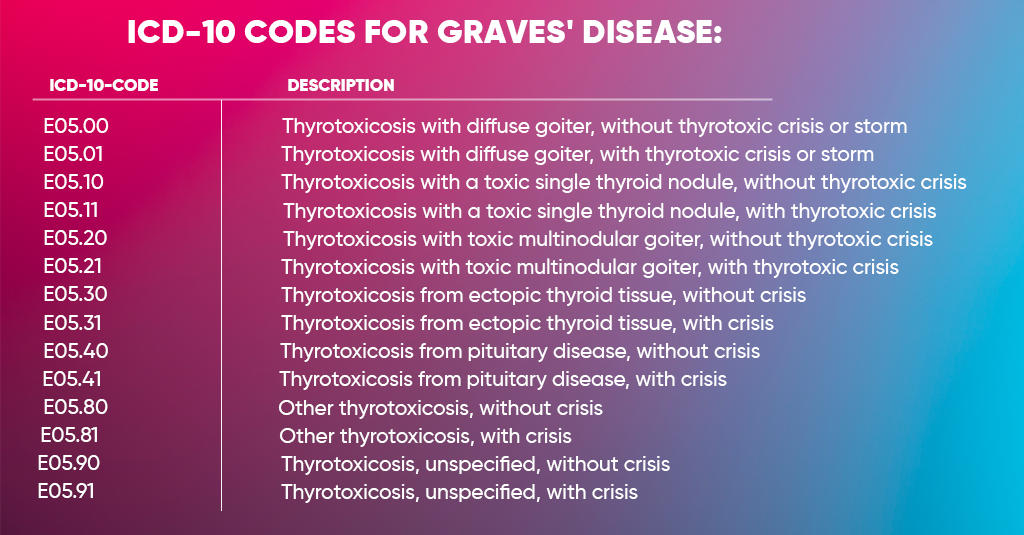
The main ICD-10 codes for Graves’ disease fall under E05.0 – Thyrotoxicosis with diffuse goiter, and its subcategories describe different manifestations.
| ICD-10 Code | Description |
| E05.00 | Thyrotoxicosis with diffuse goiter, without thyrotoxic crisis or storm |
| E05.01 | Thyrotoxicosis with diffuse goiter, with thyrotoxic crisis or storm |
| E05.10 | Thyrotoxicosis with a toxic single thyroid nodule, without thyrotoxic crisis |
| E05.11 | Thyrotoxicosis with a toxic single thyroid nodule, with thyrotoxic crisis |
| E05.20 | Thyrotoxicosis with toxic multinodular goiter, without thyrotoxic crisis |
| E05.21 | Thyrotoxicosis with toxic multinodular goiter, with thyrotoxic crisis |
| E05.30 | Thyrotoxicosis from ectopic thyroid tissue, without crisis |
| E05.31 | Thyrotoxicosis from ectopic thyroid tissue, with crisis |
| E05.40 | Thyrotoxicosis from pituitary disease, without crisis |
| E05.41 | Thyrotoxicosis from pituitary disease, with crisis |
| E05.80 | Other thyrotoxicosis, without crisis |
| E05.81 | Other thyrotoxicosis, with crisis |
| E05.90 | Thyrotoxicosis, unspecified, without crisis |
| E05.91 | Thyrotoxicosis, unspecified, with crisis |
Most Graves’ disease cases are best represented with E05.00 or E05.01, depending on whether the patient experienced a thyrotoxic crisis.
Commonly Associated ICD-10 Codes
Because Graves’ disease can trigger or accompany other complications, coders often report secondary diagnoses alongside E05.00–E05.01.
| Condition | ICD-10 Code |
| Graves’ ophthalmopathy (exophthalmos) | H05.20–H05.29 |
| Tachycardia | R00.0 |
| Anxiety disorder due to hyperthyroidism | F06.4 |
| Weight loss | R63.4 |
| Osteoporosis secondary to hyperthyroidism. | M81.8 |
Always document these comorbidities and manifestations — they help justify lab tests, imaging, and extended visits.
CPT and Procedure Codes Commonly Used
While ICD-10 codes describe the diagnosis, CPT/HCPCS codes represent what was done.
For Graves’ disease, you’ll often use a combination of evaluation, lab, and treatment codes:
| Category | Common CPT Codes | Notes |
| Office visits | 99202–99215 | Based on MDM and time |
| Thyroid function tests | 84436, 84439, 84443 | T3, T4, and TSH |
| Imaging (ultrasound, scan) | 76536, 78014 | Thyroid ultrasound or uptake scan |
| Radioactive iodine therapy | 79005, 79030 | Administered by nuclear medicine |
| Follow-up visits | 99212–99214 | Long-term management |
The Billing Process for Graves’ Disease
Let’s go through the typical end-to-end billing workflow for a Graves’ disease encounter.
Verify Patient Eligibility
Before you even run a TSH test or schedule a scan, confirm:
- The patient’s plan covers endocrine services.
- Specialist visits (endocrinology, nuclear medicine) require no pre-authorization.
- Lab networks are in place.
Most denials for thyroid workups come from unverified or expired referrals.
Code Accurately with Supporting Documentation
Use E05.00–E05.01 as your primary diagnosis.
Add secondary codes for ophthalmopathy, anxiety, or cardiac symptoms if documented.
Your Documentation should include:
- Clinical findings (tachycardia, tremors, weight loss)
- Lab results (TSH, T3, T4)
- Imaging reports (thyroid ultrasound, uptake scans)
- Treatment plans (medication, radioactive iodine, surgery)
Apply Correct CPT and Modifier Codes
If multiple services are performed the same day (e.g., exam + lab + imaging), apply modifiers such as:
- Modifier 25 – Significant, separately identifiable E/M service
- Modifier 59 – Distinct procedural service (for bundled lab/imaging)
- Modifier TC/26 – When billing for technical or professional components of imaging
Submit Claims Electronically
Most payers accept electronic submissions through:
- Availity
- Change Healthcare
- Office Ally
- Payer-specific portals (Medicare, Medicaid, BCBS, etc.)
Attach clinical documentation or lab results when required for medical necessity.
Manage Denials and Rejections
Common denial reasons:
- Non-specific diagnosis (e.g., “E05.9” used instead of “E05.00”)
- Missing modifier for multi-service days
- No documentation of thyrotoxic symptoms
Fix: Rebill with the exact ICD-10 and attach supporting reports (e.g., TSH values showing hyperthyroidism).
Reimbursement Rates and Payer Rules
Reimbursement for Graves’ disease services depends on three main factors: the payer type, the service provided, and the provider’s specialty. Each payer follows its own payment formula and documentation rules, which can affect how much you actually receive for the same visit or procedure.
Medicare (Part B)
Medicare reimburses fairly standardized rates using the Medicare Physician Fee Schedule (MPFS), which is based on Relative Value Units (RVUs). For common office visits such as CPT 99213–99214, providers typically receive between $75 and $150. Medicare payments are consistent but closely tied to proper coding and compliance. Any missing modifier or documentation gap can quickly lead to a reduced or denied claim.
Medicaid
Medicaid usually reimburses the lowest among all payers — about 60–80% of Medicare’s rates. The program enforces tighter documentation rules, especially for services involving radioactive iodine. In many states, Medicaid also requires National Drug Code (NDC) reporting for RAI-related claims. While reimbursement may be lower, Medicaid claims must still meet strict clinical and billing standards to avoid denials or recoupments.
Commercial Insurance Plans
Private payers like Blue Cross Blue Shield, Aetna, and Cigna generally pay 10–25% more than Medicare for the same Graves’ disease visits or procedures. However, they often come with extra administrative hurdles. For example, radioactive iodine (RAI) therapy or certain imaging services may require prior authorization before treatment. Providers who fail to secure this approval risk non-payment, even if the service is medically necessary.
Reimbursement depends on the payer type, service, and provider specialty.
| Payer | Typical Reimbursement Example | Notes |
| Medicare (Part B) | $75–$150 for standard office visits (99213–99214) | Uses MPFS based on RVUs |
| Commercial Plans (BCBS, Aetna, Cigna) | 10–25% higher than Medicare | Requires prior authorization for RAI therapy |
| Medicaid | Lower rates, often 60–80% of Medicare | Strict documentation and NDC requirements for radioactive iodine |
Check the Medicare Physician Fee Schedule (MPFS) for updated RVUs on endocrine services. Procedures like 79005 (radioactive iodine) and 76536 (thyroid ultrasound) are reimbursed separately if medically justified.
Documentation and Compliance Guidelines
To ensure compliance with CMS and payer audits:
- Record the etiology (autoimmune Graves’) — not just “hyperthyroidism.”
- Include lab proof (abnormal TSH, T3, T4).
- Note treatment details — medication (methimazole, propylthiouracil), RAI, or surgery.
- Document symptom progression and response to therapy.
- Use ICD-10 combination codes whenever available (don’t just code E05.9).
For Medicare claims:
- Submit E05.00 as the principal diagnosis.
- Link all labs and imaging to the same diagnosis.
- Ensure all referring providers (PCP, endocrinologist, radiologist) are NPI-linked in the claim.
- Use diagnostic test modifiers (e.g., -TC, -26) if applicable.
- Review LCDs (Local Coverage Determinations) from your MAC — some regions require proof of TSH suppression for coverage of RAI scans.
Best Practices to Maximize Reimbursement
Billing for Graves’ disease may seem routine, but small coding or documentation errors can chip away at your revenue over time. To keep payments consistent and denials low, providers should focus on a few core strategies that tighten the entire billing workflow — from coding to claim submission.
Always verify payer policies.
Before performing thyroid imaging or radioactive iodine (RAI) therapy, confirm each payer’s coverage policy and pre-authorization requirements. Commercial plans, in particular, often require prior approval for RAI or specialized imaging, so checking these details upfront saves time and prevents claim denials.
Code to the highest specificity.
Avoid using vague or “unspecified” codes like E05.9 when more accurate ones exist. For example, using E05.00 (thyrotoxicosis with diffuse goiter, without crisis) not only reflects clinical precision but also meets payer requirements for medical necessity—the more specific your diagnosis, the stronger your claim.
Attach lab results and reports.
When submitting claims for thyroid panels, imaging, or RAI therapy, include supporting Documentation — such as TSH, T3, and T4 levels, or ultrasound findings. These attachments speed up payer approval and help justify the medical necessity of your services.
Use modifiers correctly.
Modifiers can make or break a claim. Use Modifier 25 when billing an E/M visit on the same day as a procedure, or Modifier 59 to indicate distinct procedural services. For imaging, apply -26 (professional) or -TC (technical) components appropriately. Correct modifier use prevents bundling denials and ensures full payment for each service rendered.
Audit your claims monthly.
Set up a regular internal audit to track underpayments, frequent rejections, or delayed reimbursements. Patterns often reveal training gaps or coding issues. A quick monthly review can catch minor problems before they become large revenue leaks.
Train staff on autoimmune Documentation.
Graves’ disease involves detailed clinical notes — lab data, symptom progression, and treatment response. Make sure your front desk, coders, and billers understand how to document autoimmune thyroid disorders properly. Well-trained teams create cleaner claims and faster payments.
Keep fee schedules updated.
The Medicare Physician Fee Schedule (MPFS) is updated annually, and those changes affect all payers. Review and update your billing software and charge sheets regularly. Outdated rates can lead to misbilling, compliance risks, and revenue loss.
Final Thoughts
Graves’ disease coding isn’t just about typing an ICD-10.
It’s about telling the full clinical story — the autoimmune trigger, the thyroid overdrive, the lab confirmation, and the follow-up care.
When your Documentation and codes align, payers understand precisely what you treated — and they pay accordingly.
So next time you file a claim for Graves’ disease, remember:
“Code precisely. Document clearly. Bill confidently.”
Ready to Simplify Your Endocrinology Billing?
Graves’ disease billing doesn’t have to drain your staff’s time or your revenue.
The A2Z Medical Billing is here to optimize the billing and coding process for your practice.
Our team of certified medical billers handles coding, claims, denials, and reimbursements for endocrine practices nationwide — so you can focus on patient care.
Request a Free Endocrinology Billing Consultation Today