If you have ever had to bill for a preoperative clearance visit, you know it can be confusing.
- Who pays for it?
- What diagnosis codes go on the claim?
- And why do some claims get denied while others sail through?
The reality is that preoperative clearance billing is one of those areas where a small mistake can cost you a lot of money.
The rules are specific, and payers audit these claims regularly.
This guide covers everything you need to know about ICD-10 coding for pre-op clearance so you can get paid for the work you do.
What Is a Preoperative Clearance Visit?
A preoperative clearance visit is an evaluation performed by a provider to determine if a patient is healthy enough to undergo surgery. This is typically done by a primary care physician or a specialist like a cardiologist or pulmonologist.
During this visit, the provider reviews the patient’s medical history, performs a physical exam, and may order tests to assess the patient’s risk for complications during surgery. The goal is to identify any issues that could make the surgery risky and to optimize the patient’s health before the procedure.
This is different from the surgeon’s own preoperative visit. The surgeon’s visit to discuss the procedure and obtain informed consent is typically included in the global surgical package and cannot be billed separately.
The Z01.81 Code Family: Pre-Op Clearance Codes
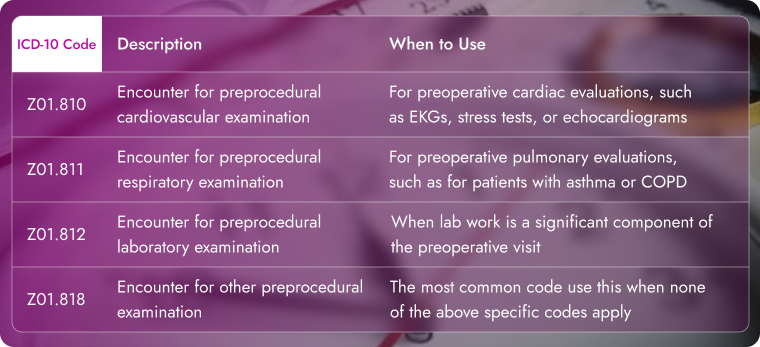
All preoperative clearance ICD-10 codes fall under the Z01.81 subcategory. These are Z codes, which are used for encounters that are not for an illness or injury but for other reasons in this case, to prepare for a procedure.
What You Need to Know?
Z01.81 is the parent code and is not billable because it lacks specificity. You must use one of the more specific codes listed above.
Correct ICD-10 Code Sequencing
Getting the order of diagnosis codes right on a claim is essential for getting paid. The primary diagnosis code tells the payer the main reason for the visit.
For a preoperative clearance visit, the correct sequence is always:
- First: The Z code from the Z01.81 family that describes the type of preprocedural examination.
- Second: The ICD-10 code for the condition that requires the surgery.
- Third (and beyond): Any additional findings or chronic conditions that were evaluated or discovered during the visit.
This order tells the payer the full story of the visit. The Z code says, “The visit was for a preprocedural exam.” The second code says, “Here is why the patient needs surgery.” The third code says, “And here is why this specific exam was medically necessary”.
Which Procedure Codes to Use
The diagnosis code is only one part of the claim. You also need the correct CPT code to reflect the service performed.
- Evaluation and Management (E/M) Codes: Use standard office visit codes (99202-99215 for new and established patients) for the clearance service. The level of E/M code depends on the complexity of the visit (history, exam, medical decision-making).
- Consultation Codes: Some commercial payers may recognize consultation codes (99241-99245), but Medicare and Medicare Advantage plans do not. For these payers, always use the standard E/M codes.
Documentation: Your documentation must clearly show that the visit was for a preprocedural evaluation and justify the level of service billed. A simple statement like “patient here for surgical clearance” is a good start, but the note should explain the decision-making process.
Billed by the Surgeon
If the patient’s own surgeon performs the preoperative history and physical, that service is considered part of the global surgical package. It is not separately billable.
Exception: If the patient develops a significant, unrelated medical condition between the decision-for-surgery visit and the surgery date, you may be able to bill a separate E/M service. You would need to document the new problem thoroughly and append modifier 25 to the E/M code.
Billed by Another Provider
When a surgeon sends a patient to a different provider (like a cardiologist or PCP) for clearance, that separate provider can bill for the service.
The key is medical necessity. The surgeon must order the clearance because the patient has a specific medical condition that needs evaluation. A routine “clearance” for a healthy patient is not medically necessary and would not support a billable visit.
Medicare’s Position: Medicare does not pay for routine preoperative clearance for surgery. However, patients with co-morbidities or other diagnoses that require additional evaluation by a professional may qualify for coverage. The evaluation must be “reasonable and necessary” for the diagnosis or treatment of an illness or injury.
What Constitutes Medical Necessity?
Understanding medical necessity is the most important part of pre-op billing. Here are the key criteria:
1. The patient has known preoperative risks. Patients with chronic illnesses such as diabetes or heart disease, especially those who are on medication that must be adjusted prior to surgery, will generally meet the criteria for medical necessity.
2. The procedure carries inherent risk. A patient with a chronic, stable condition undergoing a low-risk procedure (like cataract surgery) may not need a separate pre-op clearance. The same patient undergoing a more complicated procedure (like elective CABG) may require more detailed preoperative evaluation.
3. The surgeon requests specific advice. If the surgeon wants a recommendation on medication changes before, during, or after the surgery, this supports medical necessity.
Example of Medical Necessity: A surgeon requests a pre-op evaluation from you on a patient with chronic atrial fibrillation who is on the anticoagulant drug Coumadin. Your report discusses the physical you perform and the history you take, assesses the patient’s fitness for surgery, and makes recommendations concerning medication before, during, and after surgery. In this case, you provide specific instructions concerning the anticoagulant.
Example of No Medical Necessity: A healthy, athletic patient having minor surgery does not have a chronic disease. The preoperative evaluation that most hospitals require before surgery is generally performed by the surgeon and bundled into the global surgical package.
Documentation Requirements
Thorough documentation is the cornerstone of accurate coding and billing for preoperative visits. Here is what you need to include:
- Report to the surgeon: Provide a copy of the findings and recommendations to the requesting provider.
- The reason for the visit: Clearly states that the visit is for a preoperative evaluation at the request of the surgeon.
- Reference to the request: Mention the requesting provider’s name.
- The specific medical condition: Document the specific condition that was addressed (cardiovascular, respiratory, etc.).
- A comprehensive history and physical examination: Document the past medical history, a review of current symptoms, medications, allergies, past surgical history, and family history. Include height, weight, vital signs, and any abnormal findings.
- Risk assessment: Document your assessment of the risks associated with anesthesia, bleeding, and other potential complications.
- Medical decision-making: Explain the complexity of your decision-making process, including any discussions with the patient.
- Clearance decision: Explicitly state whether the patient is cleared for surgery and the reasons for your decision.
Billing for Preoperative Testing
Preoperative testing is another area where denials are common. Medicare will only pay for tests that are “reasonable and necessary” based on the member’s condition.
Payable tests include: Tests that are necessary based on the patient’s condition and according to National Coverage Determinations, Local Coverage Determinations, or a Priority Health Service Determination.
Not payable tests include: Routine preoperative tests that often do not meet the definition of “reasonable and necessary.” Examples include:
- Electrocardiograms or radiological tests when there is no medical indication for them
- Coagulation tests when there are no signs or symptoms of bleeding or thrombotic abnormality
- Serum iron studies when there is no indication of anemia
Real-World Coding Examples
Cardiac Pre-Op
A patient with known hypertension and a history of atrial fibrillation is scheduled for elective knee replacement surgery. The surgeon requests a cardiac clearance. The provider performs a comprehensive history, physical exam, reviews an EKG, and documents recommendations for managing Coumadin before surgery.
- Primary Diagnosis: Z01.810 (Encounter for preprocedural cardiovascular examination)
- Secondary Diagnosis: M17.11 (Unilateral primary osteoarthritis, right knee) – the reason for surgery
- Additional Diagnosis: I10 (Essential hypertension) – the condition being evaluated
- Additional Diagnosis: I48.91 (Unspecified atrial fibrillation) – the condition being evaluated
Respiratory Pre-Op
A patient with COPD is scheduled for an abdominal surgery. The pulmonologist performs a respiratory evaluation with spirometry.
- Primary Diagnosis: Z01.811 (Encounter for preprocedural respiratory examination)
- Secondary Diagnosis: K80.20 (Calculus of gallbladder without cholecystitis without obstruction)
- Additional Diagnosis: J44.1 (Chronic obstructive pulmonary disease with acute exacerbation)
Laboratory Pre-Op
A patient with diabetes is scheduled for carpal tunnel surgery. The surgeon has ordered laboratory tests as a significant component of the clearance. The evaluation includes blood work and medication review.
- Primary Diagnosis: Z01.812 (Encounter for preprocedural laboratory examination)
- Secondary Diagnosis: G56.01 (Carpal tunnel syndrome, right upper limb) – the reason for surgery
- Additional Diagnosis: E11.9 (Type 2 diabetes mellitus without complications) – the condition being evaluated
Common Billing Mistakes to Avoid
Using the Wrong Z Code
Using the general Z01.81 code is incorrect because it is not billable. You must select the specific subcode (Z01.810, Z01.811, Z01.812, Z01.818) that matches the focus of the exam.
Incorrect Code Sequencing
The Z code for preprocedural examination must be listed as the primary diagnosis. The reason for the surgery comes second. If you reverse the order, the claim will not accurately reflect the reason for the encounter.
Billing for “Routine” Clearance When Not Medically Necessary
If a surgeon sends a healthy patient for clearance with no specific medical condition to evaluate, the visit is not medically necessary. The receiving provider cannot bill for this service. This is considered an abuse of the system under Medicare rules.
Failing to Document the Medical Necessity
Your documentation must clearly state why the patient needed a preoperative evaluation. If the patient has a history of heart disease and is having major surgery, your note should explain the rationale for the cardiac evaluation. Without this link, the claim will likely be denied.
Using Consultation Codes for Medicare Patients
Many commercial payers still recognize consultation codes, but Medicare and Medicare Advantage plans do not. For these payers, always use the standard new or established patient office visit codes.
Conclusion
Billing for pre-op clearance is about precision. You need to select the correct Z code from the Z01.81 subcategory, sequence it correctly, and ensure you have the appropriate E/M CPT code.
The key to success is always the same: document medical necessity. If the patient has a chronic condition that needs evaluation before surgery, and you document it clearly, you can bill for the service. If the patient is healthy and the clearance is routine, it is not billable.
By following these guidelines, you can confidently bill for these important services and avoid unnecessary claim denials.
Need Help with Pre-Op Clearance Billing?
A2Z Medical billing team ensures your claims are coded accurately the first time, so you get paid faster and spend less time on administrative headaches.
Whether you need help with pre-op clearance billing, general coding support, or full revenue cycle management, we are here to help.
We understand the specific rules for Medicare, commercial payers, and all the nuances of documentation requirements.
Frequently Asked Questions
What is the most common ICD-10 code for a pre-op clearance visit?
The most common code is Z01.818 (Encounter for other preprocedural examination). This is used for a general pre-op evaluation when there is no specific focus on the cardiovascular, respiratory, or laboratory systems. If the exam focuses on a specific system, use the more specific code.
What CPT codes should I use for a preoperative clearance?
Use standard office or outpatient E/M codes (99202-99215) based on the level of the visit’s complexity. For Medicare patients, you should not use consultation codes (99241-99245). Some commercial payers may accept consultation codes, but Medicare does not.
Does the surgeon bill for the preoperative clearance?
No. The surgeon’s preoperative history and physical is part of the global surgical package and cannot be billed separately. The only exception is if a significant, unrelated issue develops that requires a separate visit, in which case you would append modifier 25 to the E/M code.
How should I sequence ICD-10 codes for a pre-op clearance claim?
List the Z code for the preprocedural examination first (e.g., Z01.818), followed by the code for the condition requiring surgery, and then any additional codes for chronic conditions being evaluated. This sequence accurately describes the reason for the encounter and supports medical necessity.
Does Medicare pay for preoperative clearance visits?
Yes, but only when medically necessary. Medicare does not pay for routine preoperative clearance. The patient must have a specific medical condition that requires evaluation before surgery. The evaluation must be “reasonable and necessary” for the diagnosis or treatment of an illness or injury.
What is the difference between Z01.818 and the other Z01.81 codes?
Z01.818 is the general code for other preprocedural examinations. You use it when the evaluation does not specifically focus on the cardiovascular, respiratory, or laboratory systems. The other codes (Z01.810, Z01.811, Z01.812) are used when the exam primarily focuses on those specific systems.