Neurology billing is a nightmare. Not because the work is difficult. Due to the fact that the regulations are always changing, payers engage in gamesmanship, and one minor error can cost you thousands. Claims being denied for reasons that make no clinical sense. The system is broken. However, you can still work with it.
The Medicare Cuts In 2026
As stated earlier, the 2026 Medicare physician fee schedule conversion factor has fallen to approximately $32.35 per RVU. That’s a real reduction in price for every neurology claim submitted to Medicare.
On an annual basis, per physician, you will lose somewhere between $27,000 and $82,000 in lost revenue. That’s not due to denials. That’s not due to errors. That’s the fee schedule shrinking.
Medicare Advantage plans don’t adjust their fee schedules at the same rate as traditional Medicare.
Many plans continue to pay at prior year rates for 60 to 180 days after a change, while others may reduce fees sooner.
If you’re not keeping tabs on which Payer is reducing prices, how much money you’re losing, and/or how underpaid you’ll be without knowing about it, you’re either throwing money away or getting underpaid unknowingly.
Therefore, you should conduct active Payer variance Monitoring. Your generic billing vendor isn’t likely to catch this. Neither will your in-house staff. You require someone to watch the remittance advice line-by-line.
Documentation: the monotonous item that protects your backside
Neurology claim denial rates range between 20% to 30%, nearly double the 10% to 15% national average across other specialties. Documentation deficiencies are responsible for most of those denials.
What you need to document every single Time

When documenting for Time-based billing, document the exact amount of Time. Estimates of Time are typically not acceptable. When conducting tests such as extended EEG Monitoring, track the exact number of minutes.
Do not record any Notes that may cause an audit
Here is an anecdote that will make you wince. A neurology department experienced an audit. One doctor was so far behind on Documentation that there were no Notes in the system. None whatsoever. He had to refund all the money he’d received for his services.
Another doctor billed every single visit at level 5. There was clear evidence in his Notes that supported that level of Documentation. Therefore, the department had to repay Medicare.
Record what you’ve done. Not what you wished you had done. Not what you thought you could get away with. What you actually did.
CPT coding: where most errors take place
E/M Coding
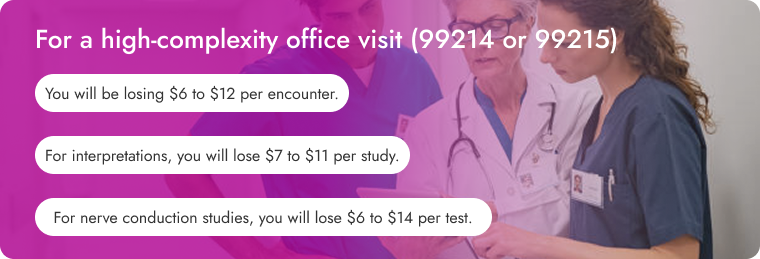
You’re likely under-documenting your e/m visits. With the 2021 transition to Medical Decision Making came opportunities. Do you see an epileptic patient come in and manage their medications, evaluate a new cognitive issue, look at an mri; and manage their hypertension? Then that’s level 5 complexity. Properly document it; bill 99215; and earn an additional $18-$28 per visit.
Several practices are leaving somewhere between $36,000 and $100,000 per physician on the table with this method alone.
EMG and NCS: don’t screw this up either
When your neurologist conducts an EMG without performing any other services, use codes 95860 – 95870 according to the body part(s) and type of study involved.
However, when NCS occur alongside EMG? The EMG is now an add-on. first, code the NCS (95907 – 95913) followed by adding:
• 95885 for limited EMG
• 95886 for complete EMG (at least five muscle groups and three nerve groups)
• 95887 for non-extremity EMG (axial muscles or cranial nerve)
Use modifier lt or RT for lateralization. Add modifier 25 to the E/M if you intend on charging for it separately.
EEG Long-Term Monitoring: know how many hours you have recorded
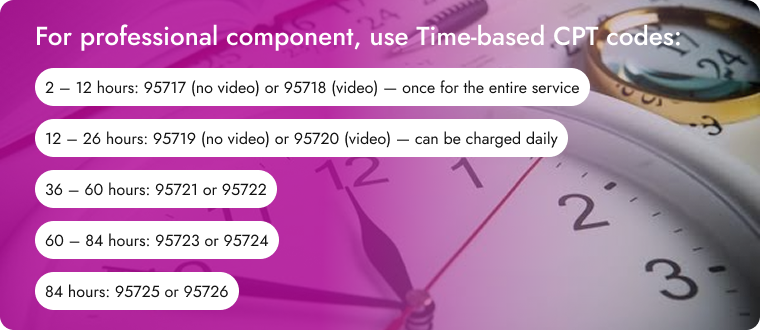
For multi-day studies, the clock starts on the day of service when you begin monitoring. Each 24-hour block gets its own code. The final partial day (2-12 hours) gets 95717 or 95718.
If you are monitoring a patient for three weeks and providing daily reports, you could charge for 95720 twenty-one times. That’s serious money.
Add-on codes: the quiet stream of lost revenue
Practices regularly fail to report add-on codes. Why? Because charge capture workflows do not prompt users to report these additional charges.
• cpt 95885/95886 for needle EMG with NCS
• CPT 95938 for short-latency somatosensory evoked potentials
• cpt 96020 for neurofunctional testing with physician oversight
These add anywhere between $40 to $90 per electrodiagnostic encounter. Those amounts are enough to offset the medicare decrease on the same procedure.
Parkinson’s disease: the entire storyline
Each Time a Parkinson’s disease patient presents, you’re utilizing codes from several different areas :
Diagnostic uses G20. Be specific. Document dyskinesia or “off episodes.” Payers prefer specificity.
First office visit utilizes e/m cpt codes 99202-99215 based upon complexity.
DaTscan imaging utilizes CPT codes 78803 (spect) or 78830 (spect/ct) plus HCPCS A9584 for the iodine injection.
Deep brain stimulation utilizes:
• 61885 for single electrode array
• 61886 for two or more arrays
• 95970-95984 for programming analysis
Therapy codes include:
• 97112 (neuromuscular re-education)
• 97116 (gait training)
• 97530 (therapeutic activities)
Speech therapy utilizes:
• 92507 (individual treatment)
• 92526 (swallowing dysfunction)
Modifiers: getting them correct
Incorrect Modifiers cause denials.
Modifier 25 goes on the E/M when you perform a procedure on the same day as the E/M. Documentation must indicate that the E/M was separately identifiable.
Modifier 26 is only used for the professional component. Technical component = TC. Some codes contain both built-in components. Identify which is which.
Modifier 59 (or XE, XS, XP, XU) indicates separate procedural services. Use it when NCCI edits bundle codes that were actually provided separately by you.
Modifier 50 is bilateral. For procedures destroying nerves, bilateral injections at the same level count as one level. If you inject both sides at multiple levels, use 64633 + modifier 50, then +64634 for each additional level without modifier 50.
Things that won’t pay you (regardless of what)
Telephones and emails services
Medicare doesn’t pay for phone calls with patients. Not as separate services. They consider this part of the payment for the office visit.
You can factor in phone Time into your next face-to-face e/m level. But document it. And don’t double-bill the same Time.
Prior authorization fees
You cannot bill for prior authorization Time. Medicare and commercial payers prohibit it. Physicians spend approximately twenty hours per week on prior authorizations, according to the American Medical Association. Uncompensated, of course.
You can bill Medicare beneficiaries directly for phone or Internet consultations if Medicare does not cover them. But get a signed advanced beneficiary notice beforehand so they know they’re paying for services without RVUs.
While CPT codes exist for almost all things, if a code has no relative value units, you won’t receive reimbursement.
Denial management: stop throwing away money
Reasons why neurology claims are denied
Top reasons:
1. Complex Documentation requirements — vague Notes lead to denials
2. Inaccurate CPT or icd-10 codes — specialty codes confuse generalists
3. Documented an incorrect amount of Time for long-term EEG and Time-based services
4. Payer-specific regulations — Medicare and commercial payers differ
5. Lack of prior authorization approval — prior approval required before rendering service
6. Bundled services error — testing bundled without appropriate Modifiers
Neurology claims also take significantly longer than other specialties to process—approximately twenty percent to forty percent longer.
How to Fix Denials?
Pre-clean your claims before submission. Automated scrubbing will find missing codes, missing Modifiers, eligibility issues, etc. Claims with ninety-five percent clean rates get processed approximately forty percent faster than dirty claims.
Quickly appeal denials. If possible, within seven days. You can recover between fifty percent to seventy five percent of lost payments by appealing quickly.
Keep track of your denial patterns — identify what continuously gets denied — address root causes rather than individual claims.
Employ certified coders — practices using specialty neurology coders reduce their denial rate by as much as fifty-four percent.
Cigna / Evernorth appeals
Submit clinical and medical necessity appeals to the Evernorth Behavioral Health Central Appeals Unit. You have one hundred eighty days from the receipt date.
UnitedHealthcare / Optum appeals
Submit via providerexpress.com — deadline is sixty-five days from adverse determination date — be aware of internal policies that conflict with generally accepted standards of care — if UnitedHealthcare denies based on an internal policy in your appeal — point out the conflict.
Aetna Appeals
Submit through Availity — deadline is one hundred eighty days from receipt date — note whether your Blue Cross plan uses Carelon Behavioral Health, Magellan, or manages BH internally — deadlines vary depending on affiliate.
The Bottom Line
Neurology medical billing requires more than generic RCM. You need someone who understands:
- Technical vs. professional components for EEG, EMG, and evoked potentials
- Time-based billing for long-term monitoring and E/M
- Bundling rules for multi-test encounters
- Documentation standards for medical necessity
- Infusion billing for MS biologics
- Prior authorization for Botox, neurostimulators, and advanced imaging
- Modifier 25 for same-day E/M and procedures
- Payer policies that change constantly
If you’re using a generic billing vendor, you’re losing money. Not because they’re bad. Because neurology is different.
The practices that survive the 2026 cuts are the ones that optimize E/M levels, capture add-on codes, recover old accounts receivable from 2024-2025 claims, and track payer variances